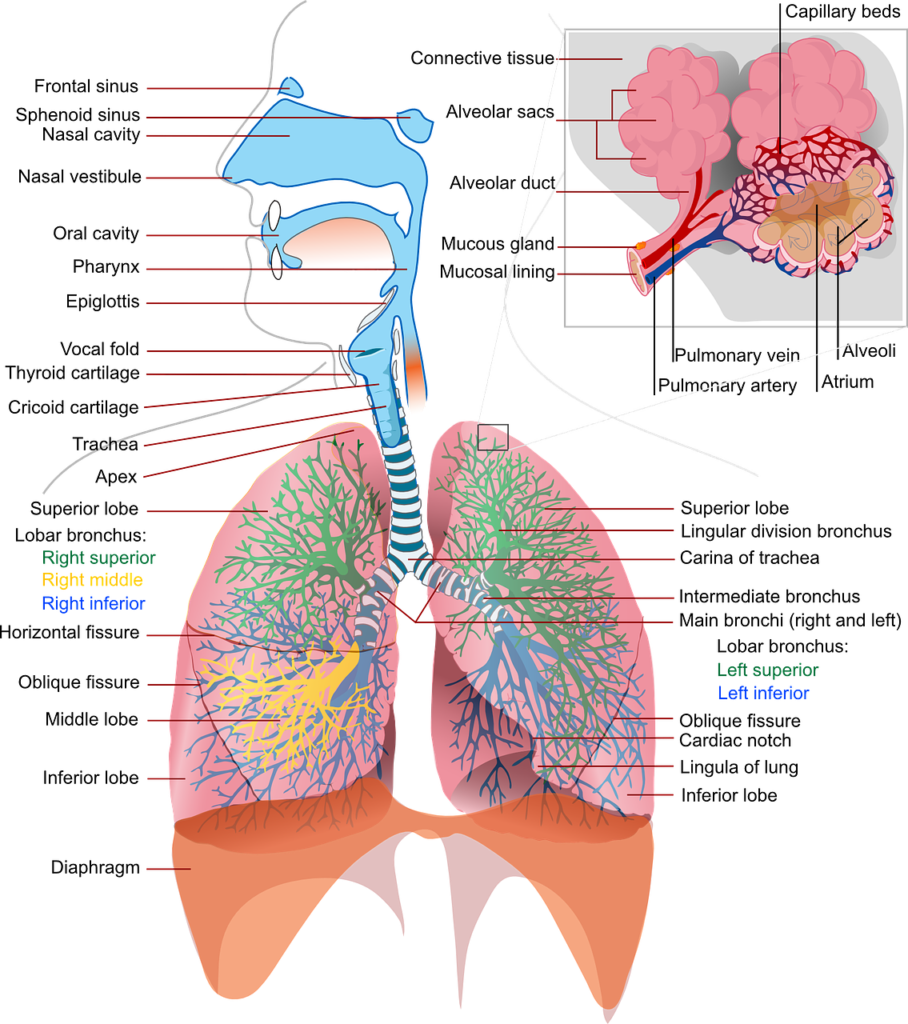
Pneumonia is a condition that results in infection of the lung parenchyma that leads to inflammation of the air sacs in one or both the lungs .
It is classified following these types :
- 1) Community acquired pneumonia
- 2) Hospital acquired
- 3) Ventilator associated
- 4) Health care associated
Pathophysology for pneumonia:
- Microorganisms, furthermore, enter the lower respiratory tract via aspiration or inhalation to the oropharynx ,hematogenous spread or an extension from a pleural space .
- Alterations in the host defense mechanism may result in overgrowth of one or more components of normal bacterial microbiota on the whole .
- Classic pneumonia presents additionally as a lobar pattern and leads to certain changes in the parenchyma :
- 1) Edema -Alveoli presents with proteinaceous exudates also .
- 2) Red hepatization – Presence of neutrophils and erythrocytes in the intra alveolar exudate
- 3) Gray hepatization – Presence of neutrophils and fibrin.
- 4) Resolution – Macrophages are especially the most dominant type
1) Community acquired pneumonia :
- Community acquired pneumonia caused due to etiologies related to bacterial infection .
- A) Typical bacterial pathogens especially like staphylococcus pneumoniae , staphylococcus aureus , haemophilus pneumoniae , klebsiella pneumoniae and pseudomonas .
- B) Atypical organisms like Mycoplasma pneumoniae , Chlamydia pneumoniae virus like influenza virus and adenovirus all in all .
- Risk factors :
- Alcoholism
- Asthma
- Immunosuppression
- Age > 70 years
- Tobacco smoking
Clinical manifestations for pneumonia:
- Patients usually present frequently with fever, chills, sweats, cough, pleuritic chest pains and also dyspnea .
- Other products following this, include nausea , vomiting , diarrhea , fatigue , headache , myalgia and arthralgia .
- Furthermore, On physical examination it reveals tachypnea (abnormal rapid breathing ) , increased or decreased tactile fremitus , dull or flat percussion and also crackles with bronchial breath sounds .
- Elderly affected faster leading to other manifestations .
Diagnosis :
Assessment and diagnosis of a critically ill or acute patients done in order to come to a conclusion as to the severity of the disease .
- A) For instance, chest x-ray to differentiate community acquired pneumonia from other conditions
- B) CT chest in patients associated with suspected cavitary disease .
- C) Sputum sampling should be done i.e. with >25 WBC and <10 squamous epithelial cells for culture .
- D) Blood cultures results up to 5-10 % of cases, hence yielding staphylococcus pneumoniae .
- E) Urine antigen tests for staphylococcus pneumoniae and legionella also are performed.
- F) PCR for nasopharyngeal swab employed method for detection of respiratory viral infection in conclusion .
Treatment :
- To decide whether the patient has to be hospitalized or not should be assessed by the following methods :
- Pneumonia severity index : Points are given especially up to 20 variables , based on age , illness , abnormal physical findings and laboratory findings .
- CURB-65 :
- Confusion
- Urea >7 mmol/l
- Respiratory rate >30/min
- Blood pressure – <90/60 mmhg
- >65 years old
- In contrast, Selecting the antibiotic therapy for the patient :
| Outpatients : |
| 1. A patient who was previously healthy and had no antibiotics for the past 3 months : a) Macrolide (Clarithromycin 500 mg BD OR Azithromycin 500 mg once , followed by 250 mg) b) Doxycycline 100 mg BD |
| 2. Comorbidities or antibiotics in the last 3 months following this : a) Fluoroquinolone ( Moxifloxacin 500 mg , Gemifloxacin 320 mg , Levofloxacin 750 mg ) or b) Amoxicillin or amoxicillin + potassium clavulanate or ceftriaxone 1-2 gm IV or cefuroxime 500mg with a macrolide |
| Inpatients , Non-ICU : |
| 1. Fluoroquinolone ( Moxifloxacin 500 mg , Levofloxacin 750 mg ) 2. Beta lactam ( Ceftriaxone 1-2 gm IV or Ampicillin 1-2 gm IV or Cefotaxime 1-2 gm IV or Ertapenem 1gm IV ) |
| Inpatient ICU : |
| 1. Beta lactam |
Complications :
- Common complications hence are as follows :
- Respiratory failure
- Shock
- Multiorgan failure
- Coagulopathy
- Myocardial Infarction
- Congestive Heart Failure
- Brain abscess
- Endocarditis
- Others like :
- Moreover, Lung abscess may occur in association with aspiration or infection caused by pathogens .
- Drainage established hence, with proper management of antibiotic therapy .
- Additionally, Pleural effusion assessment and fluid drained if the x-ray shows massive accumulation of pleural fluid
Follow up :
Chest x-ray abnormalities may require up to 4-12 weeks to heal markedly.
Additionally, for more content do visit here
Furthermore, Please refer this book for a detailed description of the disease : Harrisons book of internal medicine